
Trunk muscle activation in side plank exercises with and without external-focus instruction
Abstract
BACKGROUND:
Trunk muscle activity during isometric exercise is altered by external-focus instruction.
OBJECTIVE:
To check alterations in trunk muscle activity during side plank exercise both with and without instructions to refrain from crushing an item (external-focus instruction method).
METHODS:
Twenty-one healthy men aged 20–49 participated in this study. Ten trunk muscle activities were measured using surface electromyography during side plank exercises both with and without external-focus instruction. The unpaired t-test or Mann–Whitney U test was used to compare differences between exercise tasks and between sides.
RESULTS:
Side plank exercise with external-focus instruction increased activity of the upper trapezius, lower trapezius, latissimus dorsi, medial head of the triceps, and internal oblique on the supported side when compared with that without external-focus instruction (
CONCLUSIONS:
Adding the external-focus instruction method to the conventional side plank exercise may be effective in increasing the trunk muscles’ activity.
1.Introduction
Rehabilitation professionals have used plank (bridge) exercises to activate the trunk muscles in healthy individuals and those with low back pain [1, 2, 3]. Furthermore, trunk stability training is practical for sports performance, enhancing vertical takeoff velocity with leg strength training or combining trunk stability and leg strength training [4].
Side planks effect oblique and lumbar paraspinal recruitment and have been analyzed with and without a Swiss ball [5]. Trunk neuromuscular activity is significantly higher with additional motor task perturbations when side planks are performed on unstable surfaces compared to when performed on stable surfaces [6, 7]. Most studies have examined changes in muscle activation upon limb or position variations [3, 5].
Murofushi et al. introduced a novel isometric exercise, an external-focus instruction method performed while exerting control to avoid crushing a paper balloon maintaining a static position and holding the soft paper balloon during a chest squeeze exercise [8]. This method significantly activates the lower trapezius muscle without involving any complicated movements It causes agonist and antagonist muscle co-contraction between the lower trapezius (LT) and upper trapezius (UT), latissimus dorsi (Lat) and clavicular part of pectoralis major (PM) muscles. It is thought that adding external-focus instruction to the side plank exercise, which increases the activity of the trunk muscles [9], can induce a co-contraction and further increase the activity of the trunk muscles [8, 9]. However, no reports have examined how the activity of upper limb and trunk muscles changes when external-focus instruction is added to the side plank exercise using a paper balloon Also, no reports examine activation on the unsupported side during the side plank when external-focus instruction is added.
This study explored changes in trunk muscle activity during the side plank exercise by adding external-focus instruction for pressing a paper balloon with the palm toward the ground. This study aimed to verify whether this method can be adopted for trunk muscle activation training through side plank exercises. We hypothesized that 1) trunk muscle activity during side plank on the supported side would be significantly higher in the external-focus instruction method using paper balloons than in the conventional exercise condition, and 2) trunk muscle activity during side plank on the unsupported side would be significantly higher in the external-focus instruction method using paper balloons than in the conventional exercise condition.
2.Methods
2.1Participants
Twenty-one healthy male adults aged 20–49 participated in this study (Table 1). All participants were physically active, participated in three practice periods per week as part of a regular exercise program, and had experience in regular side plank exercise (without using a paper balloon). Before starting the experiment, participants who had a clear history of orthopedic disease within the past three months or were restricted or inhibited from participating in sports for medical reasons at the medical interview were excluded. In addition, anyone who felt pain on the examination day was excluded. The participants were instructed to stop if they felt pain during any phase of the test. None of the participants stopped treatment due to injury or pain during the examination.
Table 1
Participants’ characteristics
| Parameters | Values (interquartile range) |
|---|---|
| Number of subjects | 21 |
| Age, y | 31.3 (20–49) |
| Height, cm | 174.6 (166–189) |
| Weight, kgf | 77.6 (65–132) |
| BMI, kg/m | 25.3 (20.3–42.1) |
| Sex | |
| Male, | 21 |
BMI, body mass index;
2.2Study design
This study used a within-participant or repeated-measures design. Muscle activity was the dependent variable, and the form of exercise was the independent variable. The study was approved by the research ethics committee of the participating institution (approval number: M2019-295) on March 4, 2020 and followed the principles of the declaration of Helsinki (52nd World Medical Association General Assembly, Edinburgh, Scotland, October 2000) for medical research involving human subjects. All participants provided written informed consent for participating in the study before beginning the trials.
2.3Procedures
Side plank exercises were performed, and wireless surface electromyography (EMG) was used to analyze changes in muscle activation and its variability within the same participants and period. Muscle activation when performing the isometric method using a soft paper balloon [10] with control exerted to avoid crushing the item with the hand towards the ground was compared with that achieved by regular side plank exercise.
Table 2
Exercise setup and prescribed instructions for PBM and CSPM
| Exercise | Duration | Trials/random | Set up | Instructions |
|---|---|---|---|---|
| PBM | 10-s | 2 | Participants lie down and bear weight on one side with the shoulder abducted and elbow flexed at 90-degrees each. The wrist is pronated and extended slightly with radial deviation. The legs are split, putting the supporting side in front and the non-supporting side in the back with the toe touching the heel in front. The head, trunk, and feet were kept in a line. The hand on the non-weight-bearing side is on the pelvis with the elbow bent and relaxed | Push with maximum effort without crushing the paper balloon while maintaining the starting posture |
| CSPM | Keep the hand on the steel ball while maintaining the starting posture |
PBM, paper balloon method; CSPM, conventional side plank method.
Figure 1.
a: Paper balloon method (PBM) hand setup, b: Conventional side plank method (CSPM) hand setup, I: Right PBM, II: Left PBM, III: Right CSPM, IV: Left CSPM.
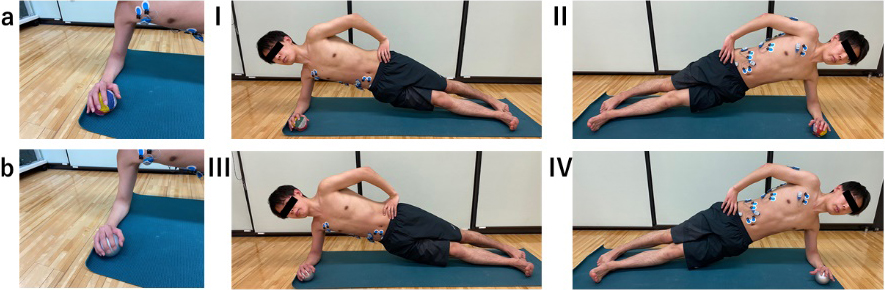
We requested the participants to keep their body position static and hold the item while exerting control to avoid crushing the soft paper balloon (Fig. 1a) and identified this activity as the paper balloon method (PBM). For the regular isometric exercise, we chose a steel ball to be placed in the hand (Fig. 1b) and identified this activity as the conventional side plank method (CSPM).
For PBM, we chose a soft paper balloon called kamifusen (UTF8min紙風船) in Japanese, a classic Japanese toy balloon with a small hole made from rice paper (configuration of the paper balloon:
2.4Trials
The participants completed four trials, with two trials each measuring muscle activities on the supported and unsupported sides of the trunk during PBM and CSPM, respectively. Each trial was conducted randomly. The continuation of the trials was regulated based on a prior study and the participants’ potential fatigue due to maximum muscle effort during the exercise task. The participants were given 90-s intervals between each performance to rest [11]. During the task, the examiner visually assessed the posture to see if it was held correctly.
The participants were instructed to remain in the same position during the side plank exercises. The participants were instructed to lie down and bear weight on one side with the shoulder abducted, elbow flexed at 90
Verbal instructions were issued to each participant before the trials to ensure proper pressing of the equipment for PBM. For PBM, participants were instructed to push without crushing the paper balloon for 10-s with maximum exertion using the supported hands to push with maximum force, being careful not to crush the paper balloon (Table 2). For PBM, the joint angle was maintained by preserving the shape of the paper balloon and the position of the hands while using maximal effort (Fig. 1-a, I, II). Participants instantly recognized when the paper balloon was crushed due to the sound of the paper collapsing, indicating when the hands were not maintaining the position. The instructions were created such that participants would focus on an external item relevant to the performed task (external-focus instruction) during the exercise.
Table 3
Placement of the EMG electrodes
| Muscle | Electrode placement location |
|---|---|
| Upper trapezius | One-half the distance between the C7 spinous process and the lateral tip of the acromion |
| Lower trapezius | 2/3 of the way up the line from the scapular spine root to the 8th thoracic vertebra |
| Latissimus dorsi | 4 cm below the lower corner of the scapula |
| Medial head of the triceps | At 50% on the line between the posterior tip of the acromion and the olecranon at 2 fingerwidths |
| medial to the line | |
| Clavicular part of pectoralis major | Medial muscle belly along the pectoralis major clavicular fibers |
| Serratus anterior | Vertically along the midaxillary line at rib levels 6 through 8 |
| External oblique | The midpoint between the ASIS and the lower end of the ribs |
| Rectus abdominis | Right aspects of the umbilicus and oriented parallel with the muscle fibers |
| Internal oblique | Approximately 2 cm medial and inferior to the ASIS |
| Multifidus | At the level of L5, on the line drawn between PSIS to L1-2 |
EMG, electromyography; ASIS, anterior superior iliac spine; PSIS, posterior superior iliac spine.
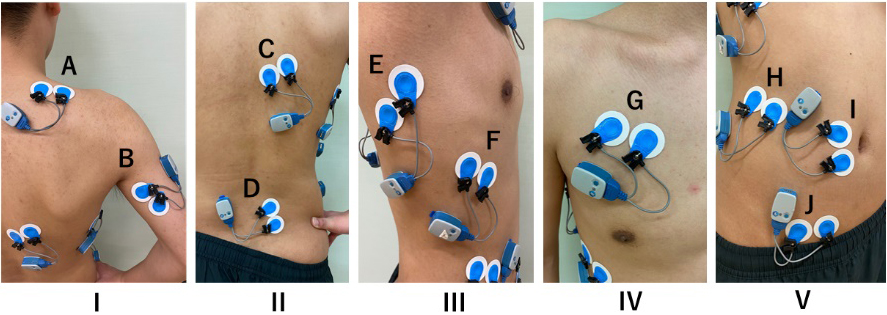
Figure 2.
The electrode application site for electromyography. I, posterior view of the upper back; II, posterior view of the lower back; III, lateral view; IV, frontal view of the chest; V, frontal view of the abdomen; A, upper trapezius; B, medial head of the triceps brachii; C, lower trapezius; D, multifidus; E, latissimus dorsi; F, serratus anterior; G, clavicular part of pectorals major; H, external oblique; I, rectus abdominis; J, internal oblique.
For CSPM, the participants were instructed to place their hands on a steel ball instead of a paper balloon, maintaining the same posture as in PBM (Fig. 1-b, III, IV).
We did not instruct participants to focus on a specific body part or muscle area (internal-focus instruction). None of the participants had experience with the PBM exercise, but each watched a video for guidance before coming to the laboratory. Furthermore, on the examination day, participants had the opportunity to experiment for 5–10-min in the laboratory to acquaint themselves with the exercises.
2.5Wireless surface EMG
Muscle activity was measured during the exercise task with surface EMG (Ultium EMG, EM-U810M8, Noraxon USA Inc., Scottsdale, AZ, USA). It was recorded at 2000 Hz with band-pass filtering (10–500 Hz) on a laptop computer (EM-P5, Noraxon) with a receiver (EM-U880, Noraxon). Before affixing the electrodes, the skin was shaved, abraded, and cleaned with alcohol. The electrode application site for EMG was determined according to prior studies [12, 13] and the guidelines of Surface ElectroMyoGraphy for the Non-Invasive Assessment of Muscles (SENIAM; http://www.seniam.org/). Surface electrodes (Ambu, Blue Sensor M-00-S, Ballerup, Denmark) were attached 35 mm apart from the UT, LT, Lat, medial head of the triceps brachii (MT), PM, serratus anterior (S Ant), external oblique (EO), rectus abdominis (RA), internal oblique (IO) and multifidus (MF) muscles on the right side. The electrodes for each muscle were precisely attached parallel to the muscle fibers (Table 3, Fig. 2). Skin impedance was verified to be less than 5 k
Table 4
The activity of each muscle in PBM and CSPM with and without support
| Muscle | Supported side [ | Unsupported side [ | ||||||
|---|---|---|---|---|---|---|---|---|
| PBM median (interquartile range) | CSPM median (interquartile range) | PBM median (interquartile range) | CSPM median (interquartile range) | |||||
| Upper trapezius | 39.95 | (35.95) | 22.65 | (23.40) | 39.25 | (48.55) | 8.36 | (2.79) |
| Lower trapezius | 77.60 | (71.75) | 27.65 | (33.35) | 137.00 | (89.35) | 34.80 | (26.40) |
| Latissimus dorsi | 166.00 | (171.50) | 69.80 | (76.70) | 93.20 | (154.35) | 13.25 | (19.73) |
| Medial head of the triceps | 130.5 | (112.60) | 38.35 | (25.25) | 71.50 | (59.45) | 3.18 | (3.80) |
| Clavicular part of pectoralis major | 50.65 | (50.00) | 25.65 | (28.50) | 76.7 | (89.20) | 12.85 | (11.34) |
| Serratus anterior | 175.50 | (82.50) | 123.50 | (100.05) | 84.2 | (43.45) | 14.55 | (17.53) |
| External oblique | 154.00 | (127.00) | 84.30 | (121.80) | 163.00 | (230.30) | 25.80 | (33.80) |
| Rectus abdominis | 94.75 | (71.45) | 53.35 | (41.75) | 48.10 | (27.35) | 14.30 | (5.46) |
| Internal oblique | 124.50 | (148.30) | 60.50 | (48.25) | 81.95 | (113.80) | 18.75 | (23.85) |
| Multifidus | 73.85 | (57.50) | 56.45 | (40.40) | 20.55 | (12.85) | 10.00 | (3.68) |
PBM, paper balloon method; CSPM, conventional side plank method.
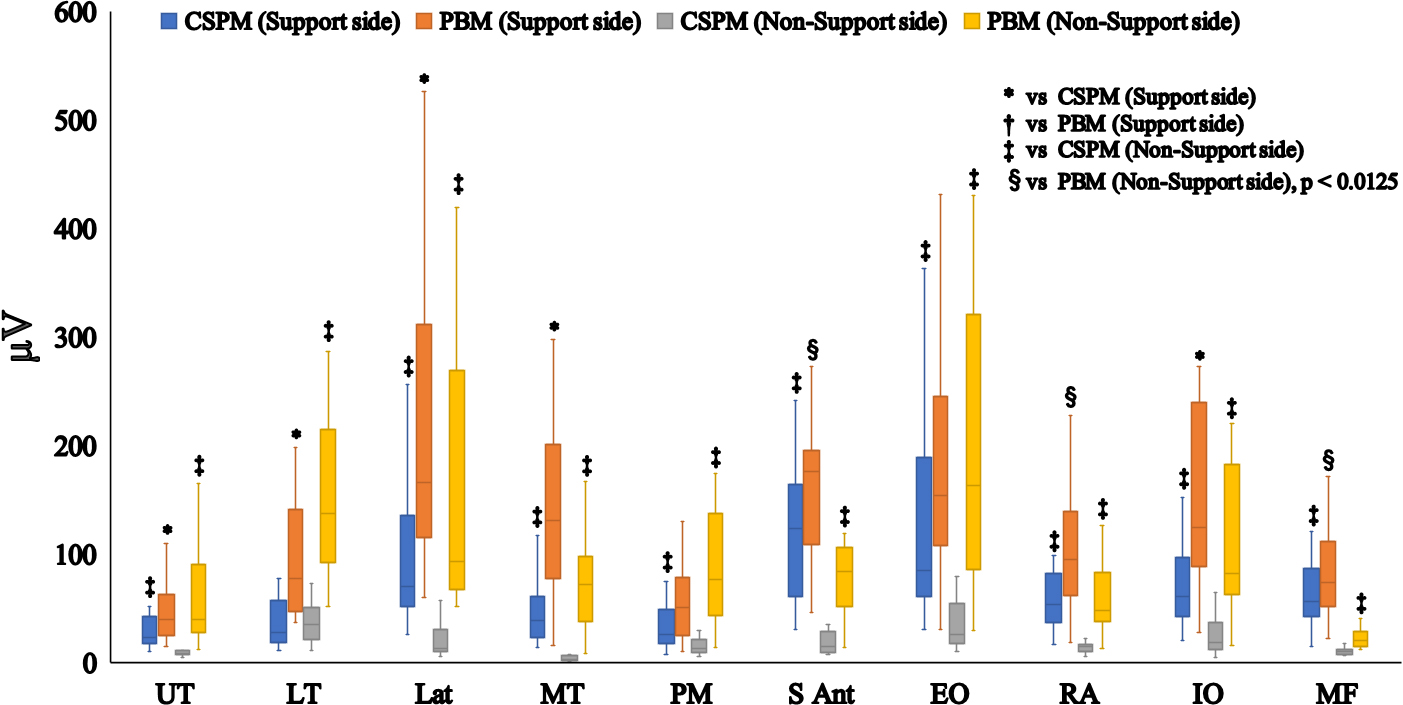
Figure 3.
Differences in muscle activity between exercise tasks. * vs CSPM (Support side),
2.6Statistical analyses
Statistical analyses were performed using IBM SPSS (version 27.0; IBM Corp., Armonk, NY, USA). The Shapiro–Wilk test was performed to determine normality. Depending on the normality of the distribution, the unpaired
3.Results
The muscle activity in each exercise and the statistical analysis results are shown in Fig. 3 and Tables 4 and 5 respectively. On the supported side, side plank exercise with external-focus instruction significantly increased activity of the upper trapezius (
Table 5
Results of the statistical analysis
| Muscles | Upper trapezius | Lower trapezius | Latissimus Dorsi | Medial head of the triceps | Clavicular part of Pectoralis Major | Latissimus Dorsi | Serratus Anterior | External Oblique| | Rectus Abdominis | Internal Oblique | Multifidus | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Experiment | Cohen’s | Cohen’s | Cohen’s | Cohen’s | Cohen’s | Cohen’s | Cohen’s | Cohen’s |
| Cohen’s |
| |||||||||||||||||||
| Supported side: CSPM vs. PBM | 0.007* | 0.916 (0.264–1.533) | 0.121 ( | 1.001 (0.342–1.623) | 1.241 (0.559–1.876) | 0.016 | 0.807 (0.163–1.419) | 1.001 (0.342–1.623) | 0.043 | 0.636 (0.004–1.243) | 0.030 | 0.605 ( | 0.026 | 0.714 (0.077–1.324) | 0.001* | 0.908 (0.256–1.525) | 0.116 | 0.496 ( | ||||||||||||
| Unsupported side: CSPM vs. PBM | 1.402 (0.703–2.049) | 0.488 ( | 1.439 (0.735–2.087) | 1.786 (1.041–2.464) | 1.615 (0.891–2.277) | 1.439 (0.735–2.087) | 1.709 (0.973–2.380) | 1.677 (0.946–2.345) | 1.838 (1.086–2.520) | 1.506 (0.795–2.160) | 1.494 (0.785–2.147) | |||||||||||||||||||
| CSPM: Supported side vs. Unsupported side | 0.870 | 0.121 ( | 0.001* | |||||||||||||||||||||||||||
| PBM: Supported side vs. Unsupported side | 0.521 | 0.463 ( | 0.017 | 0.488 ( | 0.059 | 0.016 | 0.068 | 0.566 ( | 0.059 | 0.001* | 0.697 | 0.003* | 0.125 | |||||||||||||||||
external-focus instruction. On the unsupported side, side plank exercise with external-focus instruction significantly increased activity of the upper trapezius (
4.Discussion
Compared to conventional side planks, side planks with external-focus instruction using paper balloons increased trunk muscle activity on the supported side. In addition, the activity of the trunk muscles on the unsupported side was also increased. The results of this study supported our hypothesis.
In this study, a side plank exercise was performed using a paper balloon while exerting control not to crush the item. In a previous study, Murofushi et al. demonstrated externally focused instruction while exerting control to avoid crushing an item maintaining a static position and holding a soft paper balloon during a chest squeeze exercise [8]. This method significantly activated the LT without involving any complicated movement. Furthermore agonist and antagonist muscle co-contractions were found between LT and UT, Lat and PM. The greater the force exerted by the agonist muscles, the more the appropriate amount of contraction of the antagonist muscle is required to maintain the posture and joint angle [8]. Previous studies have reported that a collection of trunk muscles work synchronously to maintain and stabilize posture [18]. Based on the above, we considered that the co-contraction of the trunk muscles during side plank exercise was further enhanced by external-focus instruction, resulting in a significant increase in the trunk muscle activity.
A previous study reported that various methods enhance side plank exercise with position changes [5, 19]. In addition, exercise on unstable surfaces is a common method of activating trunk muscles. Instability induces the muscles to react to maintain posture [6, 7]. The results of the present study provide new data in that side planks with external-focus instruction using paper balloons can increase supported and unsupported side trunk muscle activity without changing the body position.
From a clinical and rehabilitation point of view, PBM can be performed in trunk stability training for patients. Exerting control not to crush the object during side plank exercise with external-focus instruction can help train antagonist muscles by motor learning. Moreover, this method is highly convenient. Without using special tools or applying an external force using devices such as unstable elements, muscle contraction by external-focus instruction not to crush an object can produce the same effect as that with unstable conditions. Furthermore, in most rehabilitation programs, patients train with their injured arms. However, this method allows a training approach from the opposite side (i.e., non-injured arm) to avoid loading the injured arm. Therefore, this method could be widely prescribed as a new side plank exercise that can activate the trunk muscles in rehabilitation and sports settings.
This study had several limitations. First, we only examined the participants in a single position while exerting maximum effort. Different positions may lead to different muscle activation results. Second, we only measured regular side plank exercises with PBM Lastly, we did not normalize the EMG signals because data were collected and compared for the same participants during the same period within a short time [20]. Thus, these factors should be assessed and investigated in future studies
5.Conclusions
This study examined the differences in trunk muscles activity during side planks with and without external-focus instruction in healthy male subjects. The results showed that the activity of the trunk muscles on both the supported and unsupported sides increased with external-focus instruction compared to conventional side planks. Further, the differences between these muscle activations for the supported and unsupported sides were reduced. The results of this study can be used for effective training instruction for the trunk muscles.
Author contributions
CONCEPTION: Koji Murofushi.
PERFORMANCE OF WORK: Koji Murofushi, Tomoki Oshikawa, Hiroshi Akuzawa, Kenji Hirohata and Daisuke Yamaguchi.
INTERPRETATION OR ANALYSIS OF DATA: Koji Murofushi, Tomoki Oshikawa, Hidetaka Furuya and Sho Mitomo.
PREPARATION OF THE MANUSCRIPT: Koji Murofushi, Tomoki Oshikawa, Hiroshi Akuzawa, Kenji Hirohata, Daisuke Yamaguchi and Sho Mitomo.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Koji Murofushi, Tomoki Oshikawa, Hiroshi Akuzawa, Kenji Hirohata and Sho Mitomo.
SUPERVISION: Koji Murofushi, Koji Kaneoka, Kazuyoshi Yagishita and Hidetaka Furuya.
Ethical considerations
All participants provided written informed consent for participating in this study before beginning the trials. This study was approved by the research ethics committee (approval number: M2019-295, dated March 4, 2020) of the participating institution and pursuant to the principles of the Declaration of Helsinki (52nd World Medical Association General Assembly, Edinburgh, Scotland, October 2000) for medical research involving human subjects.
Funding
The authors report no funding.
Acknowledgments
We thank Editage (www.editage.jp) for English language editing.
Conflict of interest
The authors have no conflicts of interest to report.
References
[1] | Youdas JW, Coleman KC, Holstad EE, Long SD, Veldkamp NL, Hollman JH. Magnitudes of muscle activation of spine stabilizers in healthy adults during prone on elbow planking exercises with and without a fitness ball. Physiother Theory Pract. (2018) ; 34: (3): 212-222. doi: 10.1080/09593985.2017.1377792. |
[2] | Calatayud J, Casaña J, Martín F, Jakobsen MD, Colado JC, Andersen LL. Progression of core stability exercises based on the extent of muscle activity. Am J Phys Med Rehabil. (2017) ; 96: (10): 694-699. doi: 10.1097/PHM.0000000000000713. |
[3] | Okubo Y, Kaneoka K, Imai A, Shiina I, Tatsumura M, Izumi S, et al. Electromyographic analysis of transversus abdominis and lumbar multifidus using wire electrodes during lumbar stabilization exercises. J Orthop Sports Phys Ther. (2010) ; 40: (11): 743-750. doi: 10.2519/jospt.2010.3192. |
[4] | Butcher SJ, Craven BR, Chilibeck PD, Spink KS, Grona SL, Sprigings EJ. The effect of trunk stability training on vertical takeoff velocity. J Orthop Sports Phys Ther. (2007) ; 37: (5): 223-231. doi: 10.2519/jospt.2007.2331. |
[5] | Escamilla RF, Lewis C, Pecson A, Imamura R, Andrews JR. Muscle activation among supine, prone, and side position exercises with and without a Swiss ball. Sports Health. (2016) ; 8: (4): 372-379. doi: 10.1177/1941738116653931. |
[6] | Baritello O, Stoll J, Martinez-Valdes E, Müller S, Mayer F, Müller J. Neuromuscular activity of trunk muscles during side plank exercise and an additional motoric-task perturbation. Dtsch Z Sportmed. (2019) ; 70: : 153-158. doi: 10.5960/dzsm.2019.382. |
[7] | Imai A, Kaneoka K, Okubo Y, Shiina I, Tatsumura M, Izumi S, et al. Trunk muscle activity during lumbar stabilization exercises on both a stable and unstable surface. J Orthop Sports Phys Ther. (2010) ; 40: (6): 369-375. doi: 10.2519/jospt.. |
[8] | Murofushi K, Yamaguchi D, Hirohata K, Furuya H, Mitomo S. Variations in upper limb and trunk muscles activation during isometric exercise with or without exertion of control. Isokinet Exert Sci. (2022) ; 1-2. doi: 10.3233/IES-210215. |
[9] | García-Vaquero MP, Moreside JM, Brontons-Gil E, Peco-González N, Vera-Garcia FJ. Trunk muscle activation during stabilization exercises with single and double leg support. J Electromyogr Kinesiol. (2012) ; 22: (3): 398-406. doi: 10.1016/j.jelekin.2012.02.017. |
[10] | Fukumori KI. Kamifusen, the self-inflating Japanese paper balloon. Phys Today. (2017) ; 70: (1): 7879. doi: 10.1063/PT.3.3437. |
[11] | Aguilera-Castells J, Buscà B, Morales J, Solana-Tramunt M, Fort-Vanmeerhaeghe A, Rey-Abella F, et al. Muscle activity of Bulgarian squat. Effects of additional vibration, suspension and unstable surface. PLoS One. (2019) ; 14: (8): e0221710. doi: 10.1371/journal.pone.0221710. |
[12] | Ekstrom RA, Donatelli RA, Carp KC. Electromyographic analysis of core trunk, hip, and thigh muscles during 9 rehabilitation exercises. J Orthop Sports Phys Ther. (2007) ; 37: (12): 754762. doi: 10.2519/jospt.2007.2471. |
[13] | Ekstrom RA, Donatelli RA, Soderberg GL. Surface electromyographic analysis of exercises for the trapezius and serratus anterior muscles. J Orthop Sports Phys Ther. (2003) ; 33: (5): 247258. doi: 10.2519/jospt.2003.33.5.247. |
[14] | Cram JR, Kasman GS, Holtz J. Introduction to surface electromyography. Gaithersburg, MD: Aspen Publishers Inc, (1998) . |
[15] | Ekstrom RA, Bifulco KM, Lopau CJ, Andersen CF, Gough JR. Comparing the function of the upper and lower parts of the serratus anterior muscle using surface electromyography. J Orthop Sports Phys Ther. (2004) ; 34: (5): 235243. doi: 10.2519/jospt.2004.34.5.235. |
[16] | McCurdy K, O’Kelley E, Kutz M, Langford G, Ernest J, Torres M. Comparison of lower extremity EMG between the 2-leg squat and modified single-leg squat in female athletes. J Sport Rehabil. (2010) ; 19: (1): 5770. doi: 10.1123/jsr.19.1.57. |
[17] | Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. New York (NY): Lawrence Eribaum Associates, (1988) . |
[18] | McGill SM, Grenier S, Kavcic N, Cholewicki J. Coordination of muscle activity to assure stability of the lumbar spine. J Electromyogr Kinesiol. (2003) ; 13: (4): 353-359. doi: 10.1016/s1050-6411(03)00043-9. |
[19] | Youdas JW, Boor MM, Darfler AL, Koenig MK, Mills KM, Hollman JH. Surface electromyographic analysis of core trunk and hip muscles during selected rehabilitation exercises in the side-bridge to neutral spine position. Sports Health. (2014) ; 6: (5): 416-421. doi: 10.1177/1941738114539266. |
[20] | Halaki M, Ginn K. Normalization of EMG signals: to normalize or not to normalize and what to normalize to. In: Naik GR, editor. Computational intelligence in electromyography analysis – A perspective on current applications and future challenges. Rijeka: InTech Open; (2012) ; pp. 175-194. doi: 10.5772/49957. |


